Vermont Healthcare Commentary

The following commentary was sent to the Vermont House Appropriations Committee and VT Digger.
To the Editor:
Aren’t we all just tired of the Healthcare dilemma, discussion, debate, and failed attempts at political remedies in Vermont, let alone across our great nation? The Healthcare issue is huge and important, yes; but much of the national discussion around the problem seems old to most of us by now, and common perceptions have well moved beyond frustration to fatigue, or worse, indifference. After all, hasn’t the situation become one step forward (e.g., American Healthcare Act – “Obamacare”) and two steps back (e.g., another political storm, and we are still paying more than ever)? Can there ever be a fix to this expensive mess we call American Healthcare?
To be specific, the answer to that simple question is, “No, there is not a single solution to this very complicated problem.” There are paths to follow that have their own challenging, individually missioned, seemingly unrelated milestones that can be attained. Step by challenging step, achieving these milestones will lead us to a Healthcare environment that will eventually be acceptable for the majority of parties concerned.
There is a movement growing up from Vermont’s grass roots that represents the people that see one of those necessary milestones, and it has bravely entered the battle to attain it. They are on a good track. Namely, this mission is to push forward Universal Access to Primary Care. Let me explain why this is so important:
In hospitals across the country, including those in Vermont, Emergency Departments typically represent the second highest cost – the first being Intensive Care Departments. Why? Because Emergency Departments (EDs) are geared for emergent care, for trauma victims or patients that have immediate healthcare needs. EDs are staffed with highly skilled medical and supporting staff; they utilize highly technical diagnostic equipment; and they are designed to serve as an all-important gate of access into the host hospital. So, what is the problem?
Emergency Departments were formerly (and sometimes still are) referred to as “Emergency Rooms” because, as described above, they served people who needed emergent care - immediate medical attention requiring skilled medical staff and diagnostic equipment not available at the local doctor’s office. This patient population was, and still is, relatively small in the world of Healthcare delivery. (More on this later. . .) In the “old days,” there was a designated “room” where these emergent patients would be seen. However, today – as then - these emergent patients are, in reality, a small minority of the overall Healthcare patient population. The resulting problem, caused by more and more sub-acute patients being seen by EDs geared for highly acute patients, is called “over-utilization.” Quite simply, this is waste.
EDs have unfortunately become the catch-all for patients that don’t have a doctor (or insurance), cannot get an appointment to see a Primary Care doctor in time, or are mentally ill patients “delivered” to the facility. So, what was formerly an “Emergency Room,” has evolved into a complex and expensive “Emergency Department” that attempts to deal with all that is thrown at it.
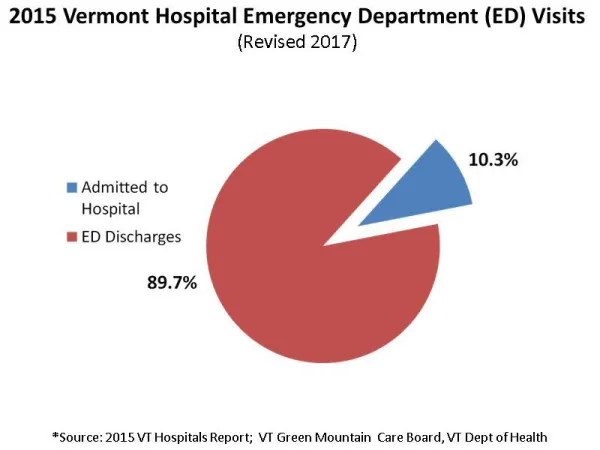
The waste of highly skilled staff time and the use of expensive equipment is extremely costly. According to the Green Mountain Care Board Report for 2015 (revised for 2017), the overall average charge for an ED visit was $2048 – significantly higher than a typical monthly mortgage or rent payment. In 2015, there were 240,356 total ED same-day discharges in Vermont that drove hospital charges of $492,148,138 – and these numbers do not include those patients that were admitted to the hospital from the ED!
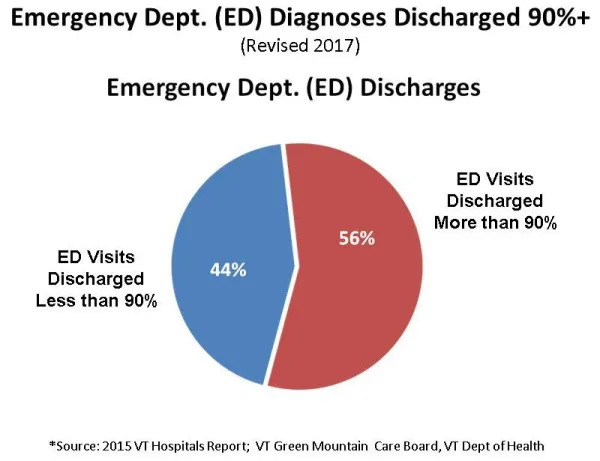
Now, let’s dig one level deeper: Nearly 60% of those Vermont ED same-day discharges represent patient treatments that are discharged over 90% of the time.
Within this group of patients, a large portion represents what is referred to as lower acuity, and have less emergent care needs. In other words, many of these people (let’s say, half) should not have to be presenting at our hospital EDs for colds, flu, rashes, or “symptoms, signs, ill-defined conditions.” Let’s all agree: the most appropriate provider to treat these patients is the Primary Care system.
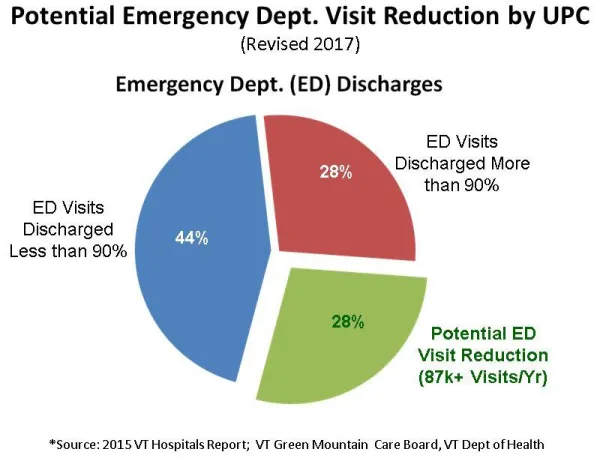
If Vermont establishes Universal Access to Primary Care, this current condition of waste in our Emergency Departments will be drastically impacted – saving Vermonters at least an estimated $40-$50 million annually.
This solution will pay for itself in a short time, and, in addition, patients struggling with chronic conditions will begin to seek less expensive care earlier. Every Vermonter wins with better access to Primary Care. There are some smart folks in Vermont right now that are working hard to get this done. For political reasons in Montpelier, Senate Bill S.53, “Universal Access to Primary Care,” is facing serious adversity from representatives and senators. However, YOU can help this bill to be passed during this legislative session. This is one of those milestones we referred to earlier that will move us toward a better Healthcare environment overall. Free primary care may sound counter-intuitive to those that aren’t privy to the larger impact; but, for the good of our Healthcare system in Vermont (and the entire nation, for that matter), this action must be taken.
I urge you to contact your local state legislators, and ask that they move the S.53 initiative forward this session.
[David Hills is the managing partner of Waypoint Management Services based in Middlebury, Vermont. He is a 25-year veteran of Healthcare consulting in over 50 Institutions across the United States.]